

Плавающая сауна отправилась в свой дебютный рейс
Парные бани популярны в Исландии, Японии, Скандинавии и других частях мира, а модный тренд Сиэтла — плавающая сауна.
Фирма goCstudio завершила строительство частной WA Sauna, и сейчас эта экстраординарная парилка плавает в городском водоёме Lake Union.
Это эксклюзивное «потогонное» заведение, площадью 240 квадратных футов было профинансировано через Kickstarter в октябре 2014 года.
Плавающая баня была завершена ровно через год, и теперь она функционирует всё время. Уникальное судно может вместить шесть человек.
Оно приводится в движение электрическим вращающимся двигателем с тремя 12-вольтовыми батареями и обогревается от дровяной печи.
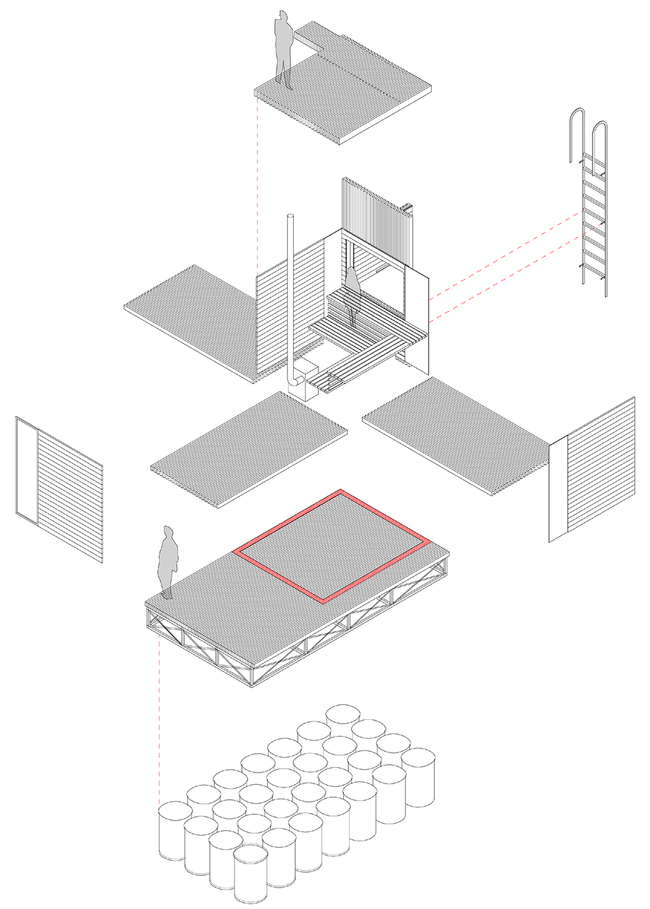
Благодаря 28 пустым 55-галлонным цилиндрам, прикреплённым снизу, обеспечивается плавный ход Конструкция сауны составляет около 7 на 7 футов и помещена на палубе 8 на 16 футов, размере стандартного прицепа.
Весит около 4500 фунтов. Окна выполнены из прозрачных акриловых панелей, а интерьер и скамейки – из еловой древесины. Снаружи все сделано из морской фанеры, экономически эффективной и удобной для транспортировки.
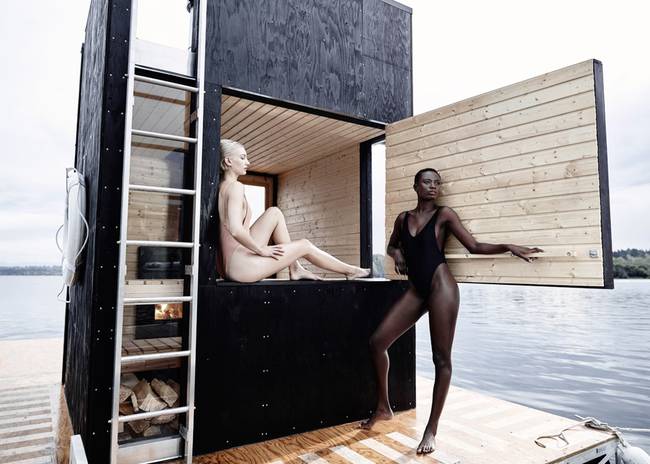
Из парилки можно легко выйти через двери или боковой люк и быстро охладиться, прыгнув в холодную воду озера

Есть платформа для дайвинга и место для солнечных ванн

Дрейфующую парную нанимают обычно на два-три часа
Хотелось бы побывать в такой сауне?





